

The International Day for the Elimination of Violence against Women marks the start of the global 16 Days of Activism against Gender-Based Violence from November 25 to December 10.
By Sahil Parmar & Shreya Anjali
Hospitals are meant to heal, yet for countless women, they become places where injuries are treated, but stories remain unheard. Bruises are dressed and fractures set, but the questions that matter most go unasked. As India advances digital health and universal coverage, it must confront the silence within the very system meant to protect women.
That silence now extends online as well, where violence follows women through their phones, social media, and messaging platforms. India faces a challenge not of policy scarcity but of policy indifference. The health system with unmatched reach through more than 1.78 Lakh Ayushman Arogya Mandirs, more than 2000 district/sub-district hospitals, and 10 lakh ASHAs could act as a lifeline for survivors. Instead, for many women, it becomes another institution where pain is processed, but not understood.
The silent epidemic
Gender-based violence remains one of India’s most entrenched public-health crises. The National Family Health Survey-5 graph shows that 32 per cent of ever-married women aged 18-49 have faced physical, sexual, or emotional spousal violence, with physical violence most common. Yet only 14 per cent of survivors seek help, and state-level data reveal stark variations across the country. Cybercrimes against women have also surged, more than doubling between 2018 and 2022, with online harassment, stalking, and image-based abuse rising rapidly. Digital spaces have become major sites of gendered harm, where abuse is anonymous, relentless, and easily amplified, blurring the boundaries of safety.
Percentage of ever-married women age 18-49 who have ever experienced spousal physical, sexual, or emotional violence]
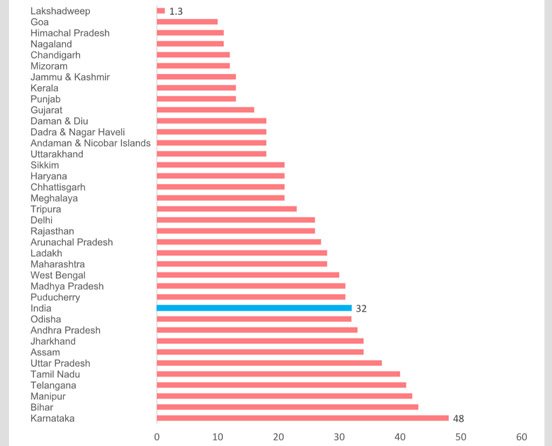
(Graph source: National Family Health Survey-5)
Globally, the WHO estimates that 1 in 3 women worldwide has faced violence from a partner. GBV (Gender-based violence) is linked to depression, anxiety, PTSD, chronic pain, and even suicide. In India, three per cent of pregnant women face violence, increasing risks of miscarriage, low birth weight and serious maternal complications.
Despite the scale, GBV often goes unnoticed in hospitals. Providers lack trauma-informed training, counselling spaces are limited and mental-health support is scarce, with only 0.75 psychiatrists per 100000 people. The system is even less equipped to recognize the psychological harm of digital abuse.
What exists and why it falls short
India has built a strong but underused policy ecosystem for addressing gender-based violence. The 2014 MoHFW medico-legal guidelines and 802 One Stop Centres provide a solid foundation, yet many centres remain urban-centric, understaffed and uneven in quality.
The Nirbhaya Fund allocates thousands of crores each year, but more than half often goes unspent due to slow approvals and weak coordination. The response to digital violence is even more fragmented, with limited forensics capacity, inadequate training, and no unified protocol for cases like cyberstalking or image-based abuse. Police, hospitals, OSCs, and shelter homes rarely coordinate, leaving survivors medically treated but seldom counselled, and survivors of online abuse face similar gaps as systems continue to treat digital and physical violence as separate forms of harm.
Cybercrimes against women have also surged, more than doubling between 2018 and 2022, with online harassment, stalking, and image-based abuse rising rapidly. (Illustration courtesy: UNICEF India)
Learning from what works: India and beyond
Some states have shown that compassionate, systematised care is possible. The Dilaasa model in Maharashtra, the Muktha centres in Karnataka, and Kerala’s Bhoomika GBV Management Centres demonstrate how hospital-based crisis units can identify survivors early and provide screening, counselling, and referrals through trained staff in outpatient, antenatal and emergency settings.
India must now build a structured, survivor-centred health response. District hospitals need clear protocols for screening, counselling, and referral, supported by private spaces for disclosure. Providers must be trained at scale, and GBV indicators incorporated into ABDM and HMIS with strong safeguards for confidentiality. As digital abuse rises, health systems should also adopt protocols for identifying and responding to technology-facilitated violence.
Mental-health support through Tele-MANAS and the District Mental Health Program must be strengthened, and key ministries must work together to anchor hospital-based GBV care units using Nirbhaya Fund resources.
.jpg)
Emotional abuse may shatter the self-worth and mental health of GBV survivors who are exposed to humiliation, threats, and controlling behaviors. (Illustration courtesy: X@WHOEMRO)
Why this matters
Violence is a powerful determinant of health, shaping every aspect of a woman’s wellbeing. Survivors are less likely to receive antenatal care, more likely to miss children’s immunizations, and face higher risks of chronic illness and poor mental health. They also struggle to stay on long-term treatments, and their families often fall deeper into poverty as health costs rise and women’s ability to work declines.
The UN’s 2025 theme, “UNiTE to End Digital Violence against All Women and Girls,” reminds us that violence in all its forms, from physical harm to online abuse, demands real investment and not just rhetoric.
The moral diagnosis
The promise of universal health coverage rings hollow if hospitals cannot offer safety to half the population they serve. Every woman who walks out unheard, whether bearing physical wounds or the quieter scars of digital abuse, reflects a profound moral and institutional failure. Violence may not begin in hospitals, but healing can when the health system chooses to ask, to listen, and to believe.
At times, the most transformative public health intervention is simply the willingness to recognise suffering in all its forms and to uphold a woman’s dignity in both the physical and digital worlds.
(Dr Sahil Parmar & Shreya Anjali are public health professionals at Pahle India Foundation, a policy think-tank based in New Delhi.)











